A1xLLcqAgt0qc2RyMz0y
Veteran
Not sure if this is faster for people to glean information.
Please provide the link to this page.
Follow along with the video below to see how to install our site as a web app on your home screen.
Note: This feature may not be available in some browsers.
Not sure if this is faster for people to glean information.
Please provide the link to this page.
If he recovers with no battling, it'll work in his favour. "See, it's just a cold."
Has any politician or celebrity died from Covid19? I feel in the common consciousness, it's still very much a 'someone else's' problem.

Which numbers are you using btw?I found the results of UK testing and they suggest the disease is less impactful than the numbers we've been seeing for months.
Therefore, the pieces of the puzzle:
Of those individuals providing blood samples, 6.3% tested positive for antibodies to COVID-19 (95% confidence interval: 4.7% to 8.1%); this equates to 1 in 16 people or 2.8 million people in England.
That's way, way lower than the 5-15% death rates coming from confirmed cases, and shows the disease has been very widespread with largely low to zero symptoms. We're looking at a 1:9 ratio of tested cases versus true cases, and 90% of infected aren't even aware they have it.
- 246,000 confirmed cases in England
- 128,00 hospital admissions across UK, so less in just England.
- 40,000 deaths in England.
- From 3 million infected that's something like 10% showing up as positive cases, 4% being hospitalised and 1% fatality.
If so, the interpretation and advice from the WHO was completely wrong. They were looking at only the tip of the iceberg above water that they could see and failed to appreciate the rest of it under water, out of sight where it wasn't doing anything, passing harmlessly from person to person. Early suggestions were asymptomatic spreaders were a tiny minority. That appears to be complete fiction and I wonder what it was based on?
The economic impact of that 1%, especially if localised to the 65+ age range, certainly changes the discussion around lockdowns.
View attachment 4253
Edit: 16% of England's population is 65 and over, so that 1% comes from only 16% of the population. Looks like 80% of the population is largely untouched. And that's heavily skewed to older ages.
Which numbers are you using btw?
for worldwide I just type COVID into google. Switch the setting to statistics on the bar and switch to Worldwide. And when you work out fatality rate it’s 4.6%
Not in random testing type scenarios. Positivity rate should help you get an idea of the type of real spread your in across the area.The fatality rate is a lot lower since a lot of infected but undiagnosed are not counted.
The detailed numbers from the Office of National StatisticsWhich numbers are you using btw?
It's not though. The asymptomatic spread of this disease is far higher than people ever knew. It's basically a fast spreader, not a slow spreader as first described. High speed propagation, low impact. We didn't know that until we had sufficient testing. Now we have hundreds of thousands of antibody tests, we see that the spread was rapid. It was the fact it spread so fast that overwhelmed the medical resources and we heard about dozens of younger people in hospital. But those young people were the outliers, a tiny fraction who are susceptible. At the same time, their peers were getting the disease without even knowing it.And when you work out fatality rate it’s 4.6%
The number of young folk with problems is actually tiny. There have been about 4000 deaths in under 65s in UK, from 3 million people. They are a small percentage of the small percentage of people who suffer from Covid19.i think looking at the runaway potential here is the greatest fear. As long as you can keep the virus in manageable numbers, everyone medicine works. It’s really when the numbers get out of hand. Even young people will start dying in higher numbers. Because there won’t be beds to treat. The resources aren’t there
I don't think there has been enough sampling to showcase your point (is just another cold germ). the study is skewed because we performed a global lockdown. All of our standard influenza (all the influenzas combined) kill typically 650K per year. CV-19 is already at 544K and those are with largely social distancing measures and lockdown mechanisms in place. Where influenza goes unchecked globally each year and only kills 650k. CV-19 has already killed 544K in half the time, with social distances, sanitization, and global lockdown mechanisms.The detailed numbers from the Office of National Statistics
Dashboard is here: https://coronavirus-staging.data.gov.uk/
Report is already linked. Lots here: https://www.ons.gov.uk/peoplepopula...onditionsanddiseases/datalist?filter=datasets
You can basically search anything on Google for Stats in the UK and get ONS reports.
It's not though. The asymptomatic spread of this disease is far higher than people ever knew. It's basically a fast spreader, not a slow spreader as first described. High speed propagation, low impact. We didn't know that until we had sufficient testing. Now we have hundreds of thousands of antibody tests, we see that the spread was rapid. It was the fact it spread so fast that overwhelmed the medical resources and we heard about dozens of younger people in hospital. But those young people were the outliers, a tiny fraction who are susceptible. At the same time, their peers were getting the disease without even knowing it.
Right now, there are 9x as many people in Brazil with Covid19 who aren't registered who don't even know they've got the disease.
The old suggestion was 80% were mild to no symptoms, 15% were severe, and 5% were critical. The UK numbers show from 3 million people, 128,000 were hospitalised. That's 4%, not 20%.
96% are mild to no symptoms.
4% need treatment. .
1% need ventilators, of which 80% are the over 65s. And in the under 65s, it's those with underlying health conditions.
Younger, healthy people are basically immune to its effects.
The number of young folk with problems is actually tiny. There have been about 4000 deaths in under 65s in UK, from 3 million people. They are a small percentage of the small percentage of people who suffer from Covid19.
Prior to the antibody testing, we only had the viral presence tests, and there we got figures like 15% mortality and a notable percentage of younger sufferers. But the actual disease was 10x more widespread than that! Every number is an order of magnitude less severe.
At this point, it looks to me like SARS-Cov2 is just another cold germ. It's new so it'll knock out the weaker population, but the rest will have it, recover, and be able to fend it off like other coronaviruses. It'll just become another part of the invisible micro-fauna we encounter harmlessly every day. I think we got hoodwinked by misinformation because we couldn't get the right data and could only base decisions on the wrong data.
I don't think that makes a difference in terms of who's affected. We have a saturation point where we don't take people in to hospital and above that, we can't count hospitalisations and a higher proportion will die from lack of treatment. However, we didn't hit that in the UK. Everyone needing to go to hospital was crammed in and counted. Hence these figures, 128,000 hospitalisations out of 3,000,000 SARS-Cov2 infected (I guess we can't count them as Covid19 as that's the name of the disease and they didn't express the disease), must be representative.I don't think there has been enough sampling to showcase your point (is just another cold germ). the study is skewed because we performed a global lockdown.
It may not be. That part needs further investigation.I don't think that makes a difference in terms of who's affected. We have a saturation point where we don't take people in to hospital and above that, we can't count hospitalisations and a higher proportion will die from lack of treatment. However, we didn't hit that in the UK. Everyone needing to go to hospital was crammed in and counted. Hence these figures, 128,000 hospitalisations out of 3,000,000 SARS-Cov2 infected (I guess we can't count them as Covid19 as that's the name of the disease and they didn't express the disease), must be representative.
The disease only affects 4% of the population, not 20%, no? How is that figure wrong?
Not sure if this is faster for people to glean information.
The death rate doesn't tell us anything without a true infection rate.It may not be. That part needs further investigation.
I think we look at Sweden for example, who chose to ignore everything. Deaths per 1 million people surpassed Italy and the US. It wasn't until they enacted stricter social distancing measures they did finally manage to bring it all the way down (they were above 100 deaths per day at peak IIRC).
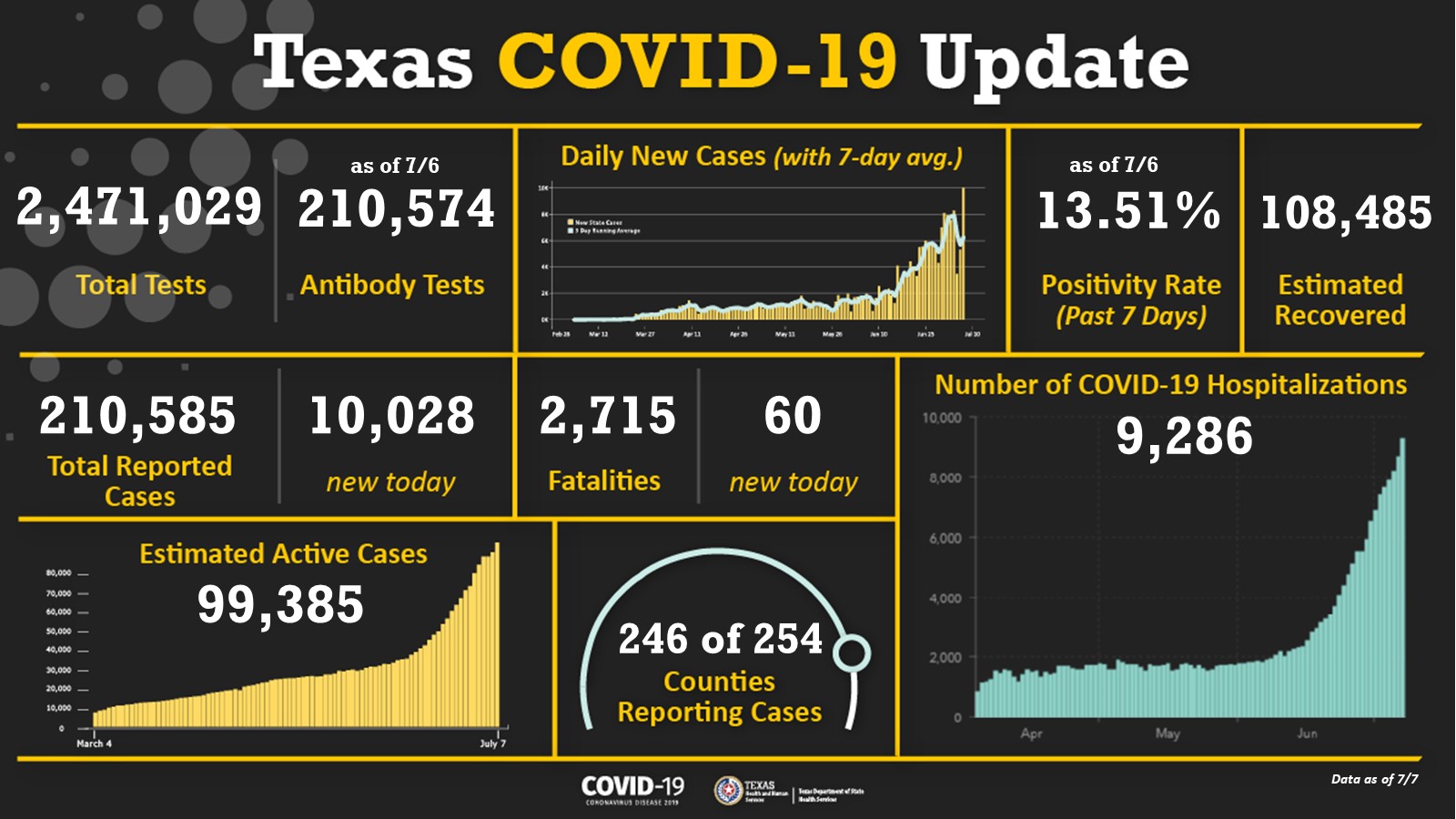
Let's say there's a virus that kills 2% of people and spreads very slowly, so over 5 years it hits everyone in a 10,000,000 population country and kills 200,000. That's ~100 people a day.And we're seeing something like that happen with unchecked Texas and Florida again. they are at 60 deaths a day now? Deaths lag behind cases, so we'll know soon enough.
The missing number is actual infection rate. All counting to date has been people going to medical services with symptoms to be tested, or medical staff, etc. associated with known cases. Some 10% of them or whatever are positive. Outside of that number is the people not being tested because there's nothing wrong with them. Antibody testing finally let's us catch up with how many people have had C19 and fills in the missing total infection rate.I can't tell you that you're wrong, the numbers suggest your summary. But that's just 1 piece of a larger puzzle, we don't know what information is missing as to why some countries fair better than others.
That's why sampling methods matters and long term sampling we will obtain a fairly reasonable representation of the reality.The death rate doesn't tell us anything without a true infection rate.
Right but with all trends and anomalies, we look at the long term run rate for those samples.The missing number is actual infection rate. All counting to date has been people going to medical services with symptoms to be tested, or medical staff, etc. associated with known cases. Some 10% of them or whatever are positive. Outside of that number is the people not being tested because there's nothing wrong with them. Antibody testing finally let's us catch up with how many people have had C19 and fills in the missing total infection rate.
The changing positivity rate shows increasing or decreasing rate of infection, but not the number of people being infected because we don't have a baseline. Let's say a State performs 1000 tests a day and finds 100 +ves for a week, The next week, they find 150 +ve, and then 200 +ves. We can see the infection rate is increasing to be twice as fast in the second week, but we don't know what that rate is. It might be those 100, 150, 200 people are all the people in the State with the virus and the virus infects 100 new people a week in week one. Or it might be that they are 50% of people and the virus infects 200 people a week. Or they may be just 10% of the total number of infected and in the first week, actually, 1000 people were infected but the 1000 tests missed 90% of them.
This will help over time.Accurate antibody tests finally gives us a count so we can find the rate over the past months and we can compare the numbers to the real rate as opposed to the small part we were seeing with the selective viral presence tests.
Where do you get your numbers from? Can I just source them for my own notebooks, I'll just showcase some interesting metrics since Texas seems worthy of doing some deep diving.This is nice for an overview but I will continue with my posts for both Dallas County (where I live) and Texas as a whole mainly because Texas has been shown to obscure what is really happening.