You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Coronavirus Pandemic (COVID-19) (SARS-CoV-2) [2020]
- Thread starter RDGoodla
- Start date
Greece
Population close to 11 million
1415 Confirmed cases
90 people in ICU
50 Deaths
We took measures very early, and people with mild symptoms where self isolating for 14 days and for that reason, we have performed relatively few tests (17350).
Thankfully we also suspended religious practices, since our older population is very religious and those church gatherings would probably be the end for them...
I'm quite certain that the actual cases are a lot higher (by a huge margin) compared to the confirmed cases, but due to social distancing our hospitals are, for the time being, coping fairly well.
Population close to 11 million
1415 Confirmed cases
90 people in ICU
50 Deaths
We took measures very early, and people with mild symptoms where self isolating for 14 days and for that reason, we have performed relatively few tests (17350).
Thankfully we also suspended religious practices, since our older population is very religious and those church gatherings would probably be the end for them...
I'm quite certain that the actual cases are a lot higher (by a huge margin) compared to the confirmed cases, but due to social distancing our hospitals are, for the time being, coping fairly well.
Not all countries even count them. The UK has no recovery numbers except an outdated and questionable 163 since March 22nd.Strangely high number of recoveries in NZ, shows that not all countries classify recoveries in the same way
Also deaths aren't counted the same way. Some countries attribute any death to Covid19 if the patient is infected, whereas other will attribute that to some underlying condition if the patient already had one. There's no standardised data so its incomparable. It's pretty frickin' useless to be honest. Apples to oranges and all that.
Last edited:
The perspectives video is interesting enough, but his assumptions, despite the lack of data which he complains about, seem to be talking down the risk. For example, saying that it is possible there might be fewer than 10,000 deaths in the US. He doesn't seem to acknowledge that the issue is likely to be the sudden influx of patients into hospitals over a few weeks instead of a few months of typical flu epidemics. Of course, it is over a week since this interview so perhaps he's changed his tune now?
I think the big difference with this illness is that it spreads so easily and silently that a hefty chunk of the population will inevitably get it so there will be a lot of deaths even if the fatality rate proves to be low. The numbers out of Italy and now coming out of Spain show how severe this could end up if measures to suppress the spread are ineffective. I think the numbers coming out of Africa and South East Asia are likely to be appalling once it really hits though the younger population of these areas will be of some help.
I think the big difference with this illness is that it spreads so easily and silently that a hefty chunk of the population will inevitably get it so there will be a lot of deaths even if the fatality rate proves to be low. The numbers out of Italy and now coming out of Spain show how severe this could end up if measures to suppress the spread are ineffective. I think the numbers coming out of Africa and South East Asia are likely to be appalling once it really hits though the younger population of these areas will be of some help.
I would argue that, even collateral should be counted, since it is a direct result of the virus.
A person that would survive a car crash, might not make it if there are no beds and no ICUs available.
And even something like an appendicitis might prove fatal if there are no doctors available to treat/diagnose because they are swamped by the outbreak...
A person that would survive a car crash, might not make it if there are no beds and no ICUs available.
And even something like an appendicitis might prove fatal if there are no doctors available to treat/diagnose because they are swamped by the outbreak...
the fatality rate is actually really high by percentage chance of death compared to other things like driving, flying, etc. 1% - 3% chance is very high. Multitudes order higher than a great deal of many other things.I think the big difference with this illness is that it spreads so easily and silently that a hefty chunk of the population will inevitably get it so there will be a lot of deaths even if the fatality rate proves to be low.
if the whole world was infected; that would be 80 million dead from the virus directly. The indirect deaths would be substantial as well.
the fatality rate is actually really high by percentage chance of death compared to other things like driving, flying, etc. 1% - 3% chance is very high. Multitudes order higher than a great deal of many other things.
if the whole world was infected; that would be 80 million dead from the virus directly. The indirect deaths would be substantial as well.
It would be more than this in Africa or other poor country...
yea there's that too. Health care is an issue for sure. Also being in a war torn country is also going to just exasperate issues with supplies etc.It would be more than this in Africa or other poor country...
That's mostly because of a labelling and cataloguing process though. A fair proportion of people who die as a result of Covid19 would have died anyway in the next few years. We'll end up with a front-loaded death toll and then a few years of lower deaths where people with cancer who were going to die of secondary infections, and old people who were going to die from flu, and people with heart conditions who were going to die from a heart attack, have died already from an acceleration to that from Covid19. Then there'll be some young people who had a bad reaction, as happens with flu, some young adults who were left out of care because of Covid19 hospital saturation, some older folk who would have been around another 10 years if not for the infection, who'd make up the most impactful casualties (not living so much on borrowed time)the fatality rate is actually really high by percentage chance of death compared to other things like driving, flying, etc. 1% - 3% chance is very high. Multitudes order higher than a great deal of many other things.
if the whole world was infected; that would be 80 million dead from the virus directly. The indirect deaths would be substantial as well.
I guess we won't be able to count the true additional deaths until some years after. When annual death rates have returned to normal, we can count how many expected deaths there would have been over those years, how many less the actual death rate is, subtract that from how many died during this pandemic, and get a number that represents people who would have lived through those years if not for Covid19.
April 1, 2020
Italy's case fatality rate from Covid-19 is markedly higher than elsewhere in the world, which is largely down to how cases are detected (Credit: Worldometer/BBC)
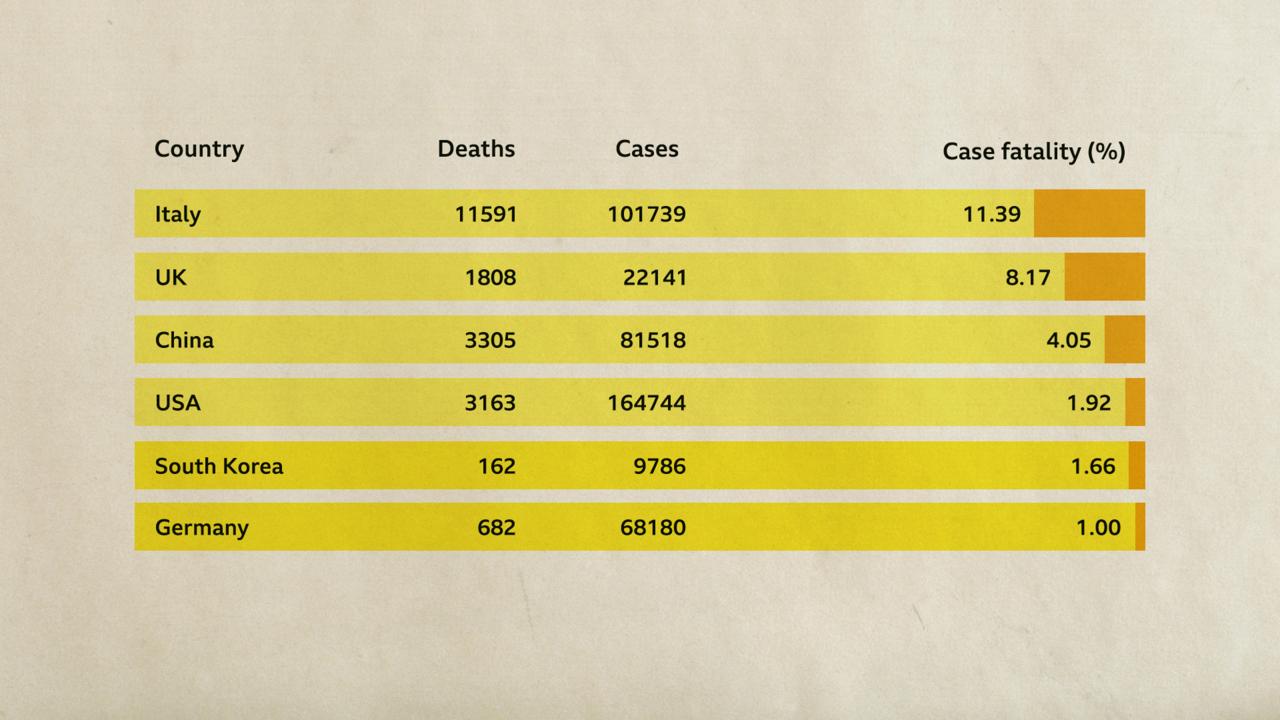
“Currently we have a huge bias in the numbers coming from different countries – therefore the data are not directly comparable,” he says. “What we need to really have valid and comparable numbers would be a defined and systematic way to choose a representative sampling frame.”
...
“If you never actually develop symptoms but had encountered the virus, that would be an infection, but it is an ‘uncountable’ one – uncountable until the time that we have an antibody test,” says Bird.
...
There are other factors that alter the death rate, too.
One of them is what doctors actually count as a Covid-19 death. At first it might seem simple enough: if a patient dies while infected with Covid-19, they died of Covid-19.
But what if they had an underlying condition, such as asthma, which was exacerbated by Covid-19? Or what if the patient died from something seemingly less related to Covid-19, which is a respiratory disease – such as, say, a brain aneurysm? Which condition should be considered the cause of death?
https://www.bbc.com/future/article/20200401-coronavirus-why-death-and-mortality-rates-differ
Italy's case fatality rate from Covid-19 is markedly higher than elsewhere in the world, which is largely down to how cases are detected (Credit: Worldometer/BBC)
“Currently we have a huge bias in the numbers coming from different countries – therefore the data are not directly comparable,” he says. “What we need to really have valid and comparable numbers would be a defined and systematic way to choose a representative sampling frame.”
...
“If you never actually develop symptoms but had encountered the virus, that would be an infection, but it is an ‘uncountable’ one – uncountable until the time that we have an antibody test,” says Bird.
...
There are other factors that alter the death rate, too.
One of them is what doctors actually count as a Covid-19 death. At first it might seem simple enough: if a patient dies while infected with Covid-19, they died of Covid-19.
But what if they had an underlying condition, such as asthma, which was exacerbated by Covid-19? Or what if the patient died from something seemingly less related to Covid-19, which is a respiratory disease – such as, say, a brain aneurysm? Which condition should be considered the cause of death?
https://www.bbc.com/future/article/20200401-coronavirus-why-death-and-mortality-rates-differ
I dont think so as the average age is a lot lower, thats part of the reason why this is getting all the media attention, its killing westernersIt would be more than this in Africa or other poor country...
I dont think so as the average age is a lot lower, thats part of the reason why this is getting all the media attention, its killing westerners
Yes but the percentage of contaminated old people dying will be much bigger. For example in Madagascar 50% of the population is under 35 years old.
There's also no obesity or diabetes, because there's not enough food for that and the sick die younger. But poor diets can mean lots of weak people. We shouldn't look to the impact on First World nations to extrapolate impact on Third World nations; there may well be different causes of death for sufferers of Covid19 in poor nations than in wealthy.I dont think so as the average age is a lot lower,...
There's also no obesity or diabetes, because there's not enough food for that and the sick die younger. But poor diets can mean lots of weak people. We shouldn't look to the impact on First World nations to extrapolate impact on Third World nations; there may well be different causes of death for sufferers of Covid19 in poor nations than in wealthy.
And this is true too younger people are not as healthy as yound people in Europe. I expect more people to die.
I don't think anyone can really know what to expect. Flu has been shown to hit poor communities hardest, but that virus is known to affect the very young as well as old. Covid19 is effectively bypassing the young. It's possible it can't be deadly to them save some outliers. It might be a disease focussed very much on 'wealthy' populations who can grow older and survive in less robust health as a result. Or not.And this is true too younger people are not as healthy as young people in Europe. I expect more people to die.
I don't think anyone can really know what to expect. Flu has been shown to hit poor communities hardest, but that virus is known to affect the very young as well as old. Covid19 is effectively bypassing the young. It's possible it can't be deadly to them save some outliers. It might be a disease focussed very much on 'wealthy' populations who can grow older and survive in less robust health as a result. Or not.
It kills weak young people too. If you have another dicease you can die. I was born in France but my parents comes from Madagascar and the health system can't handle the situation. The virus is there because of people coming from France.
That is a good point to think about though. We will find out and I had not personally considered that before you mentioned itAnd this is true too younger people are not as healthy as young people in Europe. I expect more people to die.
Statistically (although stats on this are fairly dreadful), it barely touches them. If it was killing thousands, or even hundreds, of young people, there'd be a real concern, but it's not. Even the flu can kill young healthy people. "In the last flu season, 89 children died." Spanish Flu impacted the very young with high mortality in the under 5s, whereas Covid19 is skewed very much in the upper age ranges (and perhaps mostly because these age ranges have the most underlying health conditions and pressures on good health?).It kills weak young people too.
But in the poorest nations how many such people are there who haven't died already because they can't get treatment for that condition? Here's the UK list of 'at risk':If you have another dicease you can die.
- Solid organ transplant recipients.
- People with specific cancers:
- people with cancer who are undergoing active chemotherapy
- people with lung cancer who are undergoing radical radiotherapy
- people with cancers of the blood or bone marrow such as leukaemia, lymphoma or myeloma who are at any stage of treatment
- people having immunotherapy or other continuing antibody treatments for cancer
- people having other targeted cancer treatments which can affect the immune system, such as protein kinase inhibitors or PARP inhibitors
- people who have had bone marrow or stem cell transplants in the last 6 months, or who are still taking immunosuppression drugs
- People with severe respiratory conditions including all cystic fibrosis, severe asthma and severe COPD.
- People with rare diseases and inborn errors of metabolism that significantly increase the risk of infections (such as SCID, homozygous sickle cell).
- People on immunosuppression therapies sufficient to significantly increase risk of infection.
- Women who are pregnant with significant heart disease, congenital or acquired.
It's really an unknown. LMICs have very different health states overall to wealthy countries. We only know Covid19's impact on Rich Health, not poor. Maybe their underlying health issue like malnutrition leaves them far more vulnerable, or maybe their lack of age-related health conditions means the populations will be mostly untouched?