You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Coronavirus Pandemic (COVID-19) (SARS-CoV-2) [2020]
- Thread starter RDGoodla
- Start date
So, the MHRA has authorised the use of the AstraZeneca vaccine in the UK and with a surprising twist. The half-dose/full-dose combo doesn't seem to hold up but the data seems to indicate greater efficacy if there is a longer delay between the first and second doses. Therefore, ignoring all the trial data (which is already very messy), they have decreed that as many people as possible should be given a first dose with the second to follow any time within the next 8 to 12 weeks. They've also decreed that the Pfizer vaccine should have the second dose given within 6 weeks instead of the 4 week spacing used in the trials.
Ultimately, this is an indication of just how much the shit is hitting the fan over here at present as the numbers are following the modelling with the indication that the new variant is indeed around 50% more infectious than previous strains. They reckon around 90% of all infections will be the new variant by the end of January, such is the speed of its spread. It's displacing the older strains in general circulation very quickly.
The gamble (and it is an educated gamble) is that getting the limited doses of vaccines out to the most vulnerable as quickly as possible will lead to fewer hospitalizations and deaths even if many of those receiving a vaccine don't avoid infection altogether. Probably the correct option as it is believed that just one dose should lead to at least short term protection against serious disease. Our hospitals are going to be stretched to breaking point (and perhaps further) given the surge in infections. Let's hope the rapid rollout of vaccines can reduce this as much as possible.
Ultimately, this is an indication of just how much the shit is hitting the fan over here at present as the numbers are following the modelling with the indication that the new variant is indeed around 50% more infectious than previous strains. They reckon around 90% of all infections will be the new variant by the end of January, such is the speed of its spread. It's displacing the older strains in general circulation very quickly.
The gamble (and it is an educated gamble) is that getting the limited doses of vaccines out to the most vulnerable as quickly as possible will lead to fewer hospitalizations and deaths even if many of those receiving a vaccine don't avoid infection altogether. Probably the correct option as it is believed that just one dose should lead to at least short term protection against serious disease. Our hospitals are going to be stretched to breaking point (and perhaps further) given the surge in infections. Let's hope the rapid rollout of vaccines can reduce this as much as possible.
https://thehill.com/homenews/state-...rsing-home-staff-elected-not-to-take-covid-19
Ohio Gov: 60 percent of nursing home staff elected not to take COVID-19 vaccine
About 60 percent of nursing home staff in Ohio have elected not to take the COVID-19 vaccine, Gov. Mike DeWine (R) said Wednesday.
“I’m not satisfied with where we are in Ohio," DeWine said. "We’re not moving fast enough, but we’re going to get there, and we’re going to speed this thing up.”
“We’re not going to make them, but we wish we had a higher compliance,” DeWine said. “And our message today is, [the] train may not be coming back for a while.”
Ohio has only used 14.3 percent of its vaccine allotment as of Dec. 21, The Columbus Dispatch reported, citing data from Bloomberg. The relatively slow pace comes as the U.S. is experiencing a lag between the number of vaccines distributed and the number administered.
Ohio Gov: 60 percent of nursing home staff elected not to take COVID-19 vaccine
About 60 percent of nursing home staff in Ohio have elected not to take the COVID-19 vaccine, Gov. Mike DeWine (R) said Wednesday.
“I’m not satisfied with where we are in Ohio," DeWine said. "We’re not moving fast enough, but we’re going to get there, and we’re going to speed this thing up.”
“We’re not going to make them, but we wish we had a higher compliance,” DeWine said. “And our message today is, [the] train may not be coming back for a while.”
Ohio has only used 14.3 percent of its vaccine allotment as of Dec. 21, The Columbus Dispatch reported, citing data from Bloomberg. The relatively slow pace comes as the U.S. is experiencing a lag between the number of vaccines distributed and the number administered.
Derek Lowe surveys the vaccine landscape at the end of 2020, starting with those already being deployed and those in late trials.
He's not impressed by the actions of AZ or Oxford with their vaccine.
He also says the UK is experimenting with its population, with the decision to deploy the AZ vaccine and delay the second shot but it's a reflection of the desperate state of the spread of the UK strain there. Now UK is doing the same with the Pfizer vaccine, injecting as many people as possible, potentially delaying the second shot. Pfizer has expressed that this approach hasn't been tested.
https://blogs.sciencemag.org/pipeline/archives/2020/12/30/vaccine-roundup-late-december
So having failed to control the spread, now politicians (and maybe public health authorities) are leaning heavily on the vaccines to stop the current spread, not just future spread.
He's not impressed by the actions of AZ or Oxford with their vaccine.
That situation in the UK appears to be one of the biggest factors driving the approval and rollout, and I see their point: this vaccine is indeed better than nothing, one shot for more people is likely to be better than two-shots-for-some, and it looks like they’re going to need all the help they can get. But “better than nothing” is a rough place to be. So what do we know about the efficacy of a single shot of the Oxford/AZ vaccine, and about the effect of waiting for a second one?
All I can say is that attempts to answer those questions land you immediately in a confusing mess. It’s a mess made worse by AstraZeneca, whose CEO has made statements about the vaccine’s efficacy that are not (so far) backed up by actual numbers. If you’d like me to name a major drug company that’s going to come out of this pandemic looking worse, it’s them. Anyway, as you’ll recall, initially there was a hint that a lower first dose followed by a standard second dose might be more protective overall (although I don’t think the evidence for that is very strong at all, considering the statistical spread in the data). But now there’s a report that increased efficacy might be driven by an even longer wait between the two doses. I don’t find that evidence very compelling, either (we’re getting into some pretty small subgroups by this point, and that is always a dangerous area to draw conclusions from). And if you’re going to leave people walking around with a half dose at first, or a full dose but with a longer wait for the second one, it makes the question above even more crucial: how protective is one dose?
He also says the UK is experimenting with its population, with the decision to deploy the AZ vaccine and delay the second shot but it's a reflection of the desperate state of the spread of the UK strain there. Now UK is doing the same with the Pfizer vaccine, injecting as many people as possible, potentially delaying the second shot. Pfizer has expressed that this approach hasn't been tested.
https://blogs.sciencemag.org/pipeline/archives/2020/12/30/vaccine-roundup-late-december
So having failed to control the spread, now politicians (and maybe public health authorities) are leaning heavily on the vaccines to stop the current spread, not just future spread.
To be fair, despite his criticism, Lowe does basically support the decision to space out th vaccine doses, though he notes it's only because the situation is otherwise going to be so bad.
It seems that the US are having their own problems with an almost complete failure to get the vaccines to the most vulnerable, despite the number of doses available. The fact that so many doses remain unused is mind-boggling given the circumstances.
It seems that the US are having their own problems with an almost complete failure to get the vaccines to the most vulnerable, despite the number of doses available. The fact that so many doses remain unused is mind-boggling given the circumstances.
To be fair, despite his criticism, Lowe does basically support the decision to space out th vaccine doses, though he notes it's only because the situation is otherwise going to be so bad.
It seems that the US are having their own problems with an almost complete failure to get the vaccines to the most vulnerable, despite the number of doses available. The fact that so many doses remain unused is mind-boggling given the circumstances.
Yes he's not arguing against trying to deploy as widely as possible.
But in a separate Twitter thread, he says make no mistake, this is experimentation.
I am ready and willing to get a vaccine when possible. What was with the Wisconsin person that deliberately destroyed doses of vaccine?
I haven't seen anything listing their motive. No news articles go into it.
I just don't get it. Maybe it's like the fictional joker who just wants to watch the world burn.I haven't seen anything listing their motive. No news articles go into it.
Likely some conservative anti-vaxxer nutjob?I am ready and willing to get a vaccine when possible
What was with the Wisconsin person that deliberately destroyed doses of vaccine?
I just don't get it. Maybe it's like the fictional joker who just wants to watch the world burn.
There have been cases of nurses and doctors poisoning patients. So this pharmacist may claim insanity defense.
He's lost his job, facing prison time on several felonies and probably going to lose his pharmacist license, if not be blacklisted.
You hope this is the only thing he did, because if he's willing to do something to risk the health of other people, who's to say he hasn't done something like this before?
At first I dismissed such an idea as it makes no sense. After all temperature would not affect a chip then I realized applying logic to a crazy idea is irrational so maybe you are correct. I guess we will find out whatever excuse seems best at the trial. I think that your suggestion is likely to win out whether true or not since it is more palatable to say.My guess is that he's been reading some crazy conspiracy pages and thinks he's doing people a favour by stopping the installation of the mind control chips Bill Gates has been working on all these years...
"The Imperial report on the new UK B117 strain is out. Very concerning findings, that highlight why we need to act on this *now*. These findings suggest that the situation within the UK is likely to get much worse than it is now. Here's why"
Unrolled Thread @ https://threadreaderapp.com/thread/1344774555718590464.html
---
Unrolled Thread @ https://threadreaderapp.com/thread/1344774555718590464.html
---
First, this study is perhaps one of the most comprehensive evaluations of the impact and spread of the B117 variant- combining epidemiological national evidence with genomic data from large numbers of samples across the UK.
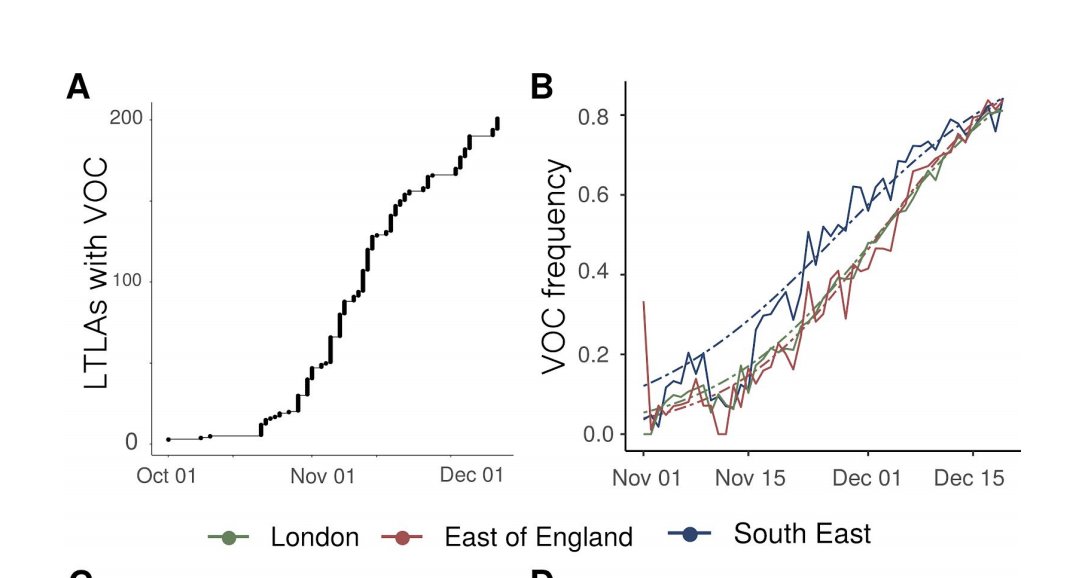
The study examines something called 'spike dropout' as a proxy indicator for the new B117 variant. The B117 variant includes a deletion in the virus genome which has been associated with a different read-out on some PCR tests, - referred to as 'spike dropout'
While 'spike dropout' (S-) does not necessarily signify the B117 variant, as this deletion can occur out with the B117 variant >97% of tests showing S- since mid-Nov have been attributed to the new variant, given it's high prevalence relative to other variants.
We see a very rapid rise in frequency of the B117 variant in London, SE England & E of England - rising to 80% by mid-Dec. Looking at the distribution across England, the estimated frequency varies by region between 15% in Yorkshire to 85% in SE England.

What does this mean?
While the variant is still at low levels across many parts of England, the trajectory in some regions (Oxford & Birmingham) suggest rapid recent increases in frequency - which means it will likely follow the same trajectory as other areas unless we act now.
Studying the Rt associated with the variant strain compared to the previous one suggests an Rt ~1.74x times greater for cases with the variant compared with the previous strain. This is a huge advantage. It would for example mean an R of 0.9 increasing to 1.6.
Worth noting that the multiplicative increase is estimated within the current context, and many not extrapolate the same way to other contexts.
Distribution of the new variant compared to the previous variant by age group suggests that the ratio between S- (variant proxy)/S+ (normal strain) is highest for those in the 0-9 yr and 10-19 yr group - data till mid-Dec. This is concerning on many levels.
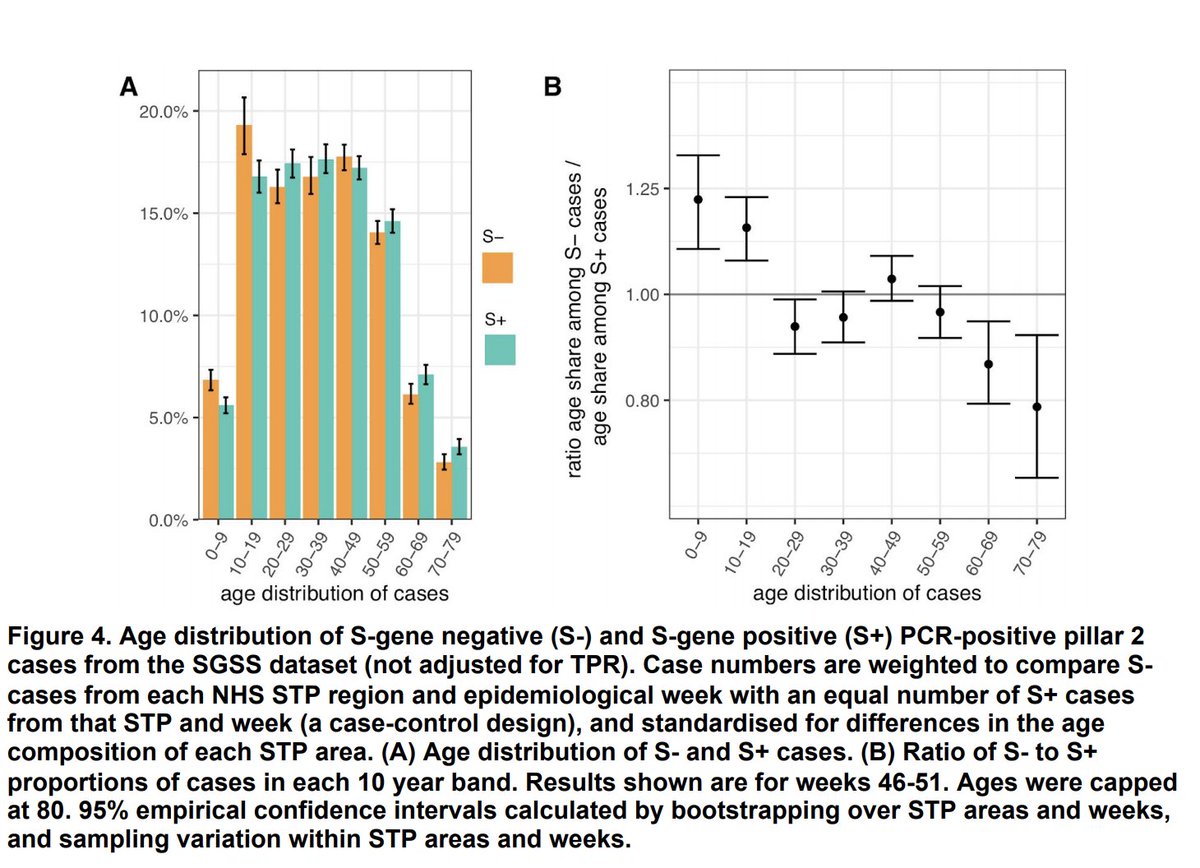
It's clear that the variant is more dominant (1.2x) in children aged 0-9 yrs and 0-19 yrs. There could be many reasons for this - including transmission dynamics - due to high levels of unmitigated transmission in schools during lockdown - which has favoured the variant.
It could also mean that children with the variant are more likely to develop symptoms and therefore be tested. Given these are not random samples from healthy people, but results based on pillar 2 testing, we need to interpret these cautiously.
This also does not necessarily mean increased biological susceptibility in children vs adults, & shouldn't be interpreted as such.
Irrespective of the relative prominence of the variant among children the prevalence of the variant is greatest among 10-19 yrs among those tested.
The data also suggests that the standard variant is still predominant among older age groups (at least among those tested) who are most susceptible to severe COVID-19.
Why is this important?
This really highlights the potential impact of waiting to act. We know that virus transmission that begins in younger age groups inevitably spreads to older people, and ultimately results in severe illness & death. We've seen this pattern before.
The geographical & age distribution suggests that although the the UK pandemic is in a critical state now, there's real potential for it to get a *lot* worse. We know increases in R correlate strongly with the variant frequency. We can see the frequency rising in other regions.
We can see it spreading outside South & East England. Given this is only at a frequency of 15% in some regions (and increasing), a rise would increase R much more than it is now, and worsen spread significantly.
Similarly, if infection in children is not curbed, the new variant will likely rapidly become dominant in adults as well, and potentially lead to even more rapid spread of infection in older groups where infection is more likely to be deadly & create further pressure on the NHS
The study shows that the R number associated with the variant *during* lockdown was 1.45 compared with 0.92 for other strains. This means that cases with the variant continued to rapidly grow during the last lockdown. The variant is associated with an increase in R of 0.4-0.7
It's clear that although the situation is dire now, there is potential for it to get much worse & given the rises we're seeing in variant frequency in other regions, if we don't act now, not only with exponential rise continue, but the rate of rise will increase.
This may also mean more cases among older age groups- while the variant is currently dominant among children, the situation is likely to get much worse if this gains dominance among adults, who will be more likely to spread to other adults & older people - which means more deaths
To illustrate this with an example-
Say 15% of a region has the variant now, and has an overall R of 1.1 (fairly realistic given the rises we're seeing in much of England where the variant isn't dominant yet).
Assuming R of 1.7 for the VOC and 1 for the standard strain, the variant would be expected to rise to >70% frequency within a month. This would mean an increase in R to 1.5 in this period from 1.1. In terms of case numbers it would be devastating.
Assuming 2000 daily cases in a region at baseline, in real terms, this would mean - 62,000 daily cases in 2 months time, vs 5,187 had the R remained constant at 1.1.
And an order of magnitude greater no. of deaths (assuming similar age distribution which may not be the case)
All the evidence is pointing in the same direction- we need to act urgently to curb spread across *all* of the UK. Letting this variant spread is not an option. And we need to close schools, until we can make them safe, & prevent onward transmission. This is critical now.
Full report here: https://www.imperial.ac.uk/media/im...2020-12-31-COVID19-Report-42-Preprint-VOC.pdf
Just adding a short note here as many people have asked how the variant increases transmissibility. We don't know the exact mechanism -we know that one of the mutations changes the virus spike protein in a way that it binds to the human receptor needed for infection more strongly
There are also studies that suggest that virus levels in the throat and nose are higher among those infected with the virus, suggesting that this might be one of the ways in which it may make spread easier.
The study examines something called 'spike dropout' as a proxy indicator for the new B117 variant. The B117 variant includes a deletion in the virus genome which has been associated with a different read-out on some PCR tests, - referred to as 'spike dropout'
While 'spike dropout' (S-) does not necessarily signify the B117 variant, as this deletion can occur out with the B117 variant >97% of tests showing S- since mid-Nov have been attributed to the new variant, given it's high prevalence relative to other variants.
We see a very rapid rise in frequency of the B117 variant in London, SE England & E of England - rising to 80% by mid-Dec. Looking at the distribution across England, the estimated frequency varies by region between 15% in Yorkshire to 85% in SE England.
What does this mean?
While the variant is still at low levels across many parts of England, the trajectory in some regions (Oxford & Birmingham) suggest rapid recent increases in frequency - which means it will likely follow the same trajectory as other areas unless we act now.
Studying the Rt associated with the variant strain compared to the previous one suggests an Rt ~1.74x times greater for cases with the variant compared with the previous strain. This is a huge advantage. It would for example mean an R of 0.9 increasing to 1.6.
Worth noting that the multiplicative increase is estimated within the current context, and many not extrapolate the same way to other contexts.
Distribution of the new variant compared to the previous variant by age group suggests that the ratio between S- (variant proxy)/S+ (normal strain) is highest for those in the 0-9 yr and 10-19 yr group - data till mid-Dec. This is concerning on many levels.
It's clear that the variant is more dominant (1.2x) in children aged 0-9 yrs and 0-19 yrs. There could be many reasons for this - including transmission dynamics - due to high levels of unmitigated transmission in schools during lockdown - which has favoured the variant.
It could also mean that children with the variant are more likely to develop symptoms and therefore be tested. Given these are not random samples from healthy people, but results based on pillar 2 testing, we need to interpret these cautiously.
This also does not necessarily mean increased biological susceptibility in children vs adults, & shouldn't be interpreted as such.
Irrespective of the relative prominence of the variant among children the prevalence of the variant is greatest among 10-19 yrs among those tested.
The data also suggests that the standard variant is still predominant among older age groups (at least among those tested) who are most susceptible to severe COVID-19.
Why is this important?
This really highlights the potential impact of waiting to act. We know that virus transmission that begins in younger age groups inevitably spreads to older people, and ultimately results in severe illness & death. We've seen this pattern before.
The geographical & age distribution suggests that although the the UK pandemic is in a critical state now, there's real potential for it to get a *lot* worse. We know increases in R correlate strongly with the variant frequency. We can see the frequency rising in other regions.
We can see it spreading outside South & East England. Given this is only at a frequency of 15% in some regions (and increasing), a rise would increase R much more than it is now, and worsen spread significantly.
Similarly, if infection in children is not curbed, the new variant will likely rapidly become dominant in adults as well, and potentially lead to even more rapid spread of infection in older groups where infection is more likely to be deadly & create further pressure on the NHS
The study shows that the R number associated with the variant *during* lockdown was 1.45 compared with 0.92 for other strains. This means that cases with the variant continued to rapidly grow during the last lockdown. The variant is associated with an increase in R of 0.4-0.7
It's clear that although the situation is dire now, there is potential for it to get much worse & given the rises we're seeing in variant frequency in other regions, if we don't act now, not only with exponential rise continue, but the rate of rise will increase.
This may also mean more cases among older age groups- while the variant is currently dominant among children, the situation is likely to get much worse if this gains dominance among adults, who will be more likely to spread to other adults & older people - which means more deaths
To illustrate this with an example-
Say 15% of a region has the variant now, and has an overall R of 1.1 (fairly realistic given the rises we're seeing in much of England where the variant isn't dominant yet).
Assuming R of 1.7 for the VOC and 1 for the standard strain, the variant would be expected to rise to >70% frequency within a month. This would mean an increase in R to 1.5 in this period from 1.1. In terms of case numbers it would be devastating.
Assuming 2000 daily cases in a region at baseline, in real terms, this would mean - 62,000 daily cases in 2 months time, vs 5,187 had the R remained constant at 1.1.
And an order of magnitude greater no. of deaths (assuming similar age distribution which may not be the case)
All the evidence is pointing in the same direction- we need to act urgently to curb spread across *all* of the UK. Letting this variant spread is not an option. And we need to close schools, until we can make them safe, & prevent onward transmission. This is critical now.
Full report here: https://www.imperial.ac.uk/media/im...2020-12-31-COVID19-Report-42-Preprint-VOC.pdf
Just adding a short note here as many people have asked how the variant increases transmissibility. We don't know the exact mechanism -we know that one of the mutations changes the virus spike protein in a way that it binds to the human receptor needed for infection more strongly
There are also studies that suggest that virus levels in the throat and nose are higher among those infected with the virus, suggesting that this might be one of the ways in which it may make spread easier.
I dont know what is going on with this Covid-19. I get the impression that the measurements and the reports are a bit off.
So I got sick 30th of Nov. I went to the doctor 1st of Dec. Finds no symptoms for Covid. She found other symptoms so covid was ruled out.
10th of December me, my mother and sister do a rapid test.
Mom and sis are found positive. I am found negative. I am perfectly fine. Me and my sister have no symptoms. Mom had flu symptoms for a week. She is 65, diabetic, has high pressure, she is allergic and has some heart issues. Flu passed like a normal flu. She is fine.
I keep my distances btw just in case. My sis does a PCR test the next day to confirm if it it's false positive or not. Results come in 15th. She is still positive.
12th I meet some friends at their house and one belongs to the sensitive groups.
I move to a new place from the 13th and barely have any conduct with sis and mom or with anyone else.
17th I am called to do a PCR test the next day. I do it, they call me at the 20th and tell me I am positive. No symptoms nothing. Surprisingly my chronic cough also vanished. I sent a list of all the people that had conduct with me since the 16th to call for a PCR test and I include those I met at the 12th just in case. None has symptoms, none seems to be positive.
None seems to have Covid.
Nothing adds up.
So I got sick 30th of Nov. I went to the doctor 1st of Dec. Finds no symptoms for Covid. She found other symptoms so covid was ruled out.
10th of December me, my mother and sister do a rapid test.
Mom and sis are found positive. I am found negative. I am perfectly fine. Me and my sister have no symptoms. Mom had flu symptoms for a week. She is 65, diabetic, has high pressure, she is allergic and has some heart issues. Flu passed like a normal flu. She is fine.
I keep my distances btw just in case. My sis does a PCR test the next day to confirm if it it's false positive or not. Results come in 15th. She is still positive.
12th I meet some friends at their house and one belongs to the sensitive groups.
I move to a new place from the 13th and barely have any conduct with sis and mom or with anyone else.
17th I am called to do a PCR test the next day. I do it, they call me at the 20th and tell me I am positive. No symptoms nothing. Surprisingly my chronic cough also vanished. I sent a list of all the people that had conduct with me since the 16th to call for a PCR test and I include those I met at the 12th just in case. None has symptoms, none seems to be positive.
None seems to have Covid.
Nothing adds up.
BioNTech said that it's "highly likely" that their vaccine will work on the UK strain, because 99% of the proteins in that strain is the same as those on the earlier more widespread strains.
They also said the immunity after just one shot would last 21 days. They are really trying to discourage the UK with their 1 shot approach.
As for the AZ and adenovirus vector vaccines, we should have data about the J&J vaccine by the end of the month. The Sputnik and one of the Chinese vaccines are adenovirus vectors but nobody in the West is trusting their data, though it's being rolled out in some developing nations.
They also said the immunity after just one shot would last 21 days. They are really trying to discourage the UK with their 1 shot approach.
As for the AZ and adenovirus vector vaccines, we should have data about the J&J vaccine by the end of the month. The Sputnik and one of the Chinese vaccines are adenovirus vectors but nobody in the West is trusting their data, though it's being rolled out in some developing nations.
green.pixel
Veteran
None seems to have Covid.
Nothing adds up.
It seems that current tests are not good enough to be reliable.